Article: Silver, Ian A., Dole, Jenna L., and Semenza, Daniel C. 2026. “US Medicaid Spending and Health Insurance Coverage for People Involved in the Criminal Legal System as Children.” Medical Care, 00:000–000. https://doi.org/10.1097/MLR.0000000000002330
1. Background (PDF)
Individuals who have contact with the criminal legal system (CLS) before age 18 face serious, long-lasting barriers to health care upon reentry. Adolescent involvement in the CLS strains family and partner relationships, limits future work opportunities, and places individuals at a financial disadvantage, restricting access to private health insurance. As a result, these individuals often do not possess health insurance or rely on Medicaid as their primary source of health insurance. Briefly, Medicaid is a federal-state joint program that provides health insurance coverage to adults and children with limited income and resources, including people with disabilities. Federal and state Medicaid expenditures are extremely important for ensuring individuals with CLS contact before 18 have the opportunity to enroll in and maintain health insurance throughout adulthood.
Nevertheless, the 2025 federal budget reconciliation bill (HR1, or the “One Big Beautiful Bill Act”) proposed sweeping cuts to federal Medicaid expenditures, introducing work requirements of at least 80 hours of qualifying activities per month, and reducing insurance subsidies. These changes are projected to increase the number of uninsured Americans by approximately 7.6 million, with socioeconomically marginalized groups being impacted the most, including those with CLS involvement before the age of 18.
Despite the importance of Medicaid for this population, no prior research had examined how changes in federal and state Medicaid expenditures affect insurance enrollment among individuals involved in the CLS before 18. The current study forecasted the potential impact of increased or decreased federal Medicaid spending on uninsurance amongst formerly CLS-involved youth. The findings of which have important policy implications for federal and state legislatures, as well as local juvenile justice practitioners.
2. Results
The study yielded three findings:
First, greater CLS involvement before age 18 was associated with higher odds of being uninsured as an adult. Compared to individuals with no CLS contact, those arrested before 18 had nearly double the odds of being uninsured, and those incarcerated in a juvenile or adult facility had nearly triple the odds. Second, higher federal and state Medicaid spending was associated with lower rates of uninsurance. A $100 billion increase in federal Medicaid spending corresponded to a 20% decrease in the odds of having no insurance.
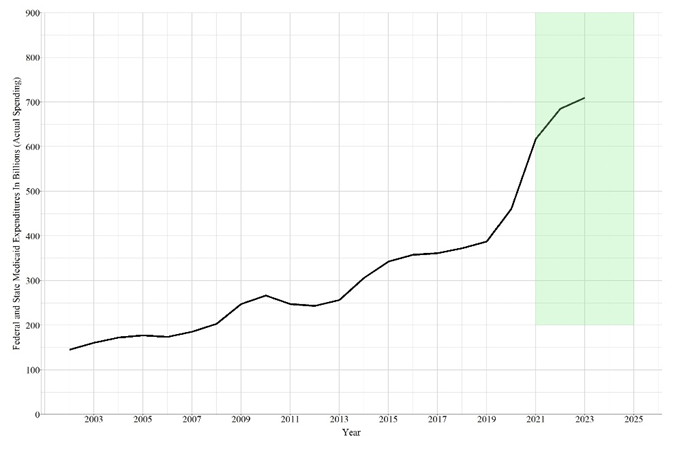
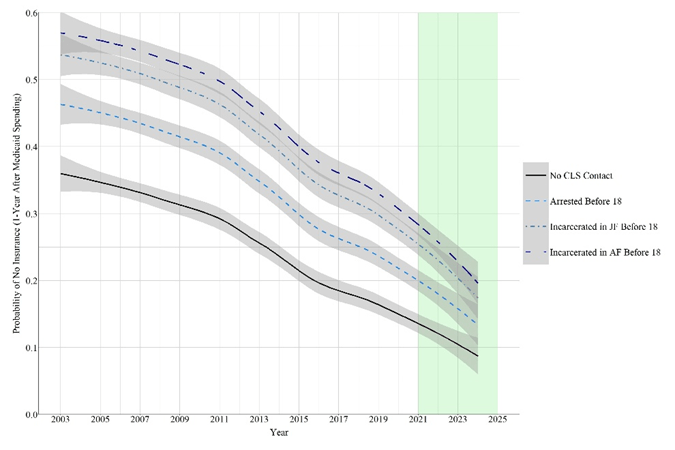
Notes: The green area represents the period after NLSY97 data collection (2021-2024). Using the real Federal Medicaid spending identified in Figure 1, a 20 percent increase in Federal Medicaid spending was calculated for 2021-2023 by adding 20 percent to the real Federal Medicaid spending amount. “No CLS contact” indicates that the individual was not arrested or incarcerated before 18, “JF” indicates juvenile facility, “AF” indicates adult facility. The predictions are based on 400 black males with 22 observations each (2002-2023 for predictors; 2003-2024 for outcome), while continuous constructs were set equal to the mean of the construct. Federal Medicaid spending each year from 2002-2023 was used to generate the predictions for the subsequent year (2003-2024). The probability of having no insurance was calculated by pulling 1,000 draws from the posterior distribution for every observation of an individual and averaging across the drawn values.
Third, the forecasts suggested that a 50% federal Medicaid cut could increase uninsurance across all groups (no CLS contact, arrested, incarcerated in juvenile facility, and incarcerated in adult facility), while widening the health insurance coverage gap between CLS-involved youth and non-CLS involved youth. In contrast, a 20% increase in federal Medicaid spending would reduce uninsurance for all groups and narrow the health insurance coverage gap (See Figure 1).
3. Implications
These findings have implications for practitioners and policymakers working at the intersection of juvenile justice, public health, and Medicaid policy:
For juvenile justice practitioners, the study reinforces existing evidence that formerly incarcerated youth have a high risk of losing, or never having health, insurance during adulthood. Contact with the CLS before 18 places individuals at a disadvantage and suggests that health care navigators could be provided to youth while going through court proceedings and during the reentry process. Briefly, health care navigators are staff who can guide youth through the application process, explain eligibility, and connect them to community health providers.
In addition to health care navigators, correctional facilities should provide health focused transitional programs for youth, educating them about the process of maintaining health insurance, and identifying and seeking care for acute or chronic health conditions.
For state Medicaid administrators and health policy professionals, they should continue to fund and conduct outreach to youth previously involved in the CLS and fully embrace the requirements of the Consolidated Appropriations Act (CCA) of 2023. Legislatures should also seek to expand Medicaid requirements for CLS involved youth, providing fundings to maintain a continuity of care and health focused treatment for this vulnerable population.
For federal policymakers, this study offers compelling quantitative evidence that federal Medicaid spending directly reduces uninsurance amongst this vulnerable population. Cutting federal Medicaid would not only increase uninsurance broadly but would disproportionately harm individuals involved in the CLS before 18. Increasing federal Medicaid investment, on the other hand, would reduce the insurance gap and advance health equity in the United States.
4. Data and Methods
This study used data from the NLSY97, a nationally representative U.S. birth cohort of 8,984 individuals born between 1980 and 1984 and followed from 1997 to 2021. The analytical sample comprised 8,240 individuals with at least four valid insurance observations, yielding 115,360 total observations. Federal and state Medicaid expenditure data were drawn from the National Health Expenditure Accounts provided by the Centers for Medicare and Medicaid Services.
Participants were classified into four mutually exclusive CLS groups based on involvement before age 18: no CLS contact, arrested only, incarcerated in a juvenile facility, or incarcerated in an adult facility. The study used a Bayesian lagged random-intercept logistic regression model (adjusting for 18 covariates) to assess associations between Medicaid spending and uninsurance. Posterior predictions then simulated the effects of a 50% federal Medicaid cut and a 20% increase across 400 identical cases. Results were stratified by race and sex, with Black males as the primary focus given their disproportionate CLS exposure before 18; findings for Black females, White males, and White females are reported as supplemental analyses.
5. Conclusion
This study delivers timely evidence suggesting federal Medicaid spending influences health insurance disparities among people involved in the CLS before 18. Individuals with prior CLS involvement, especially those incarcerated in juvenile or adult facilities, face elevated odds of being uninsured during adulthood, and Medicaid is often the only way to obtain health insurance coverage.
The proposed federal Medicaid cuts under HR1 could increase uninsurance amongst this group of vulnerable individuals and contribute to negative health outcomes (e.g., functional limitations, psychological symptoms, mortality). Expanding federal Medicaid investment would increase health care coverage amongst individuals involved in the CLS before 18
Practitioners and policymakers should use these findings to advocate for Medicaid funding, advance pre-release enrollment programs in CLS settings, and invest in health care navigation services that connect formerly CLS-involved youth to the coverage they need. Future research should examine state-level variation in Medicaid expenditures and identify targeted interventions that can interrupt the relationship between adolescent CLS involvement and adult health insurance disparities.
Disclosure: This research brief was prepared by Microsoft Copilot and reviewed/edited by Ian A. Silver.
