Article: Silver, Ian A., Tosto, Samantha A., Newsome, Jamie, and McKay, Alicia d. 2026. “Adulthood Health Insurance Source for Previous Criminal Legal System Involved Pediatrics.” Health Services Research, 61:e70106. https://doi.org/10.1111/1475-6773.70106
1. Background (PDF)
Individuals involved in the criminal legal system (CLS) before age 18 face wide-ranging collateral consequences upon reentry into the community. These include lower socioeconomic status, reduced employment opportunities, and limited access to health care. CLS-involved youth already experience elevated rates of mental health conditions, substance use disorders, and chronic illness – yet their health care needs frequently go unaddressed upon reentry.
Having health insurance is critical to affording health care in the United States. Without health insurance, some medications and procedures could cost as much as 100 times the insured rate. Notably, however, individuals with prior CLS contact during adolescence have higher rates of uninsurance (80% to 90% uninsured) when compared to the general population (do we have this?). Compounding this, formerly CLS-involved youth often have low health literacy and limited reentry support to help them navigate the enrollment process.
Despite the well-documented wellness needs of this population, relatively little research has examined the long-term effects of adolescent CLS-involvement on the source of one’s health insurance during adulthood. This study addresses this gap by investigating whether being arrested, incarcerated in a juvenile facility, or incarcerated in an adult facility before age 18 affects the number of years an individual is covered by different types of health insurance during adulthood.
2. Results
Using the National Longitudinal Survey of Youth 1997 (NLSY97) and a quasi-experimental analytical strategy, the study produced several key findings:
- Individuals with CLS involvement before age 18 had more years without health insurance.
- Youth arrested before 18 experienced a 27% increase in the number of years without health insurance. Youth incarcerated in a juvenile facility before 18 experienced a 50% increase in the number of years without health insurance.
- Youth incarcerated in an adult facility before 18 experienced a 85% increase in the number of years without health insurance.
- CLS involvement before 18 was also associated with more years covered by Medicaid (Federal/state-funded health insurance) and fewer years with employer-provided health insurance, family member-provided health insurance, and/or self-purchased health insurance.
Together, these findings indicate that CLS involvement before age 18 – particularly incarceration in adult facilities – substantially narrows the pathways to private health insurance, leaving this population more reliant on public programs or being uninsured during adulthood.

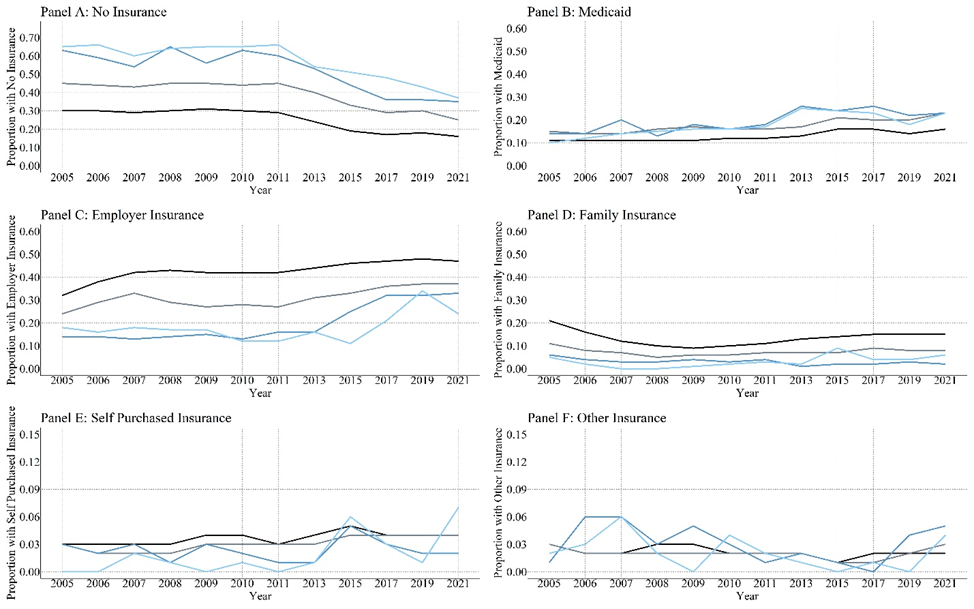
Notes: These frequencies and percentages represent the pre-imputation numbers. The number of individuals reporting health insurance source declined over time within each group. A group comparison on no health insurance was assessed using an ANOVA and a Tukey’s post-hoc evaluation.
3. Implications
These findings call for targeted policy and practice responses at the intersection of juvenile justice and health care. For juvenile justice practitioners, the CLS represents a critical intervention point. Because incarcerated youth often rely on the juvenile justice system as their primary source of medical care, facilities are well-positioned to deliver health insurance education and enrollment support. Integrating health care navigators into juvenile CLS settings could increase health literacy and facilitate continuity of health care upon reentry. Expanding Medicaid eligibility to begin 30 days prior to release and extend 90 days post-release could further reduce insurance gaps during the vulnerable transition period.
The reduced access to employer-provided insurance among CLS-involved youth also reflects broader employment barriers tied to criminal records. However, policymakers can implement laws to help youth obtain private health insurance through employers. For example, policymakers could lower the minimum number of employees required for an employer to provide health insurance coverage or could reduce the number of hours an employee has to work to be considered full-time. Moreover, policymakers could encourage employers to hire formerly CLS-involved adolescents by providing a tax credit. Additional policies that support workforce reintegration – including expungement, ban-the-box initiatives, and employer incentive programs – may help address this downstream insurance gap.
4. Data and Methods
This study used data from the National Longitudinal Survey of Youth 1997 (NLSY97), a nationally representative U.S. birth cohort of 8,984 individuals born between 1980 and 1984 and followed from 1997 to 2021. The final analytical sample comprised 7,826 individuals who were under age 18 at baseline and had at least five valid responses to health insurance items.
Participants were classified into four mutually exclusive CLS groups: no contact before age 18, arrested only before 18, incarcerated in a juvenile facility before 18, and incarcerated in an adult facility before 18. The primary outcomes were the number of years between 2005 and 2021 that respondents held each of six insurance types: no insurance, Medicaid, employer-provided, family member-provided, self-purchased, and other insurance.
Gradient boosted inverse probability weights (IPWs) for the Average Treatment Effect (ATE) were estimated using the TWANG package in R to balance 25 confounding variables across the four CLS groups. These weights were then applied in Poisson regression models predicting years with each insurance source. Missing covariate data were handled with random forest imputation.
5. Conclusion
This study demonstrates that involvement in the CLS before age 18 is associated with long-term reductions in access to private health insurance and increased reliance on Medicaid or no insurance during adulthood. These effects are largest for youth who were incarcerated in adult facilities, underscoring the importance of limiting youth exposure to the adult CLS. Given the high prevalence of physical and mental health needs among CLS-involved youth, the compounding effects of uninsurance represent a serious public health concern. Action is needed to expand Medicaid access during reentry, embed health care navigation services within juvenile justice settings, and remove policy barriers that limit formerly CLS-involved individuals from accessing employer-based coverage. Future research should examine how specific interventions can interrupt the relationship between adolescent CLS involvement and adult health insurance disparities.
Disclosure: This research brief was prepared by Claude and reviewed/edited by Ian A. Silver, Samantha A. Tosto, Jamie Newsome, and Alicia d. McKay.
