Article: Silver, Ian A., Semenza, Daniel C., and Testa, Alexander. 2026 “Pediatric Criminal Legal System Involvement and Functional Limitations in Early Adulthood.” Academic Pediatrics. 103241. https://doi.org/10.1016/j.acap.2026.103241.
1. Background (PDF)
Contact with the criminal legal system (CLS) during childhood can have lasting impacts on health and well-being. While more than 400,000 children were arrested in 2020, the long-term health consequences remain poorly understood. Prior research shows that children involved with the CLS face heightened risks of poor health outcomes, including depressive symptoms and early death. However, a critical gap exists in understanding how different forms of CLS involvement before 18 – arrest, incarceration in juvenile, or adult facilities – affect functional limitations during early adulthood. Functional limitations refer to difficulties performing everyday tasks such as climbing stairs, doing chores, working, or visiting friends. These limitations can significantly shape ones’ quality of life, employment, and social relationships. A key mechanism linking youth CLS involvement to poor adulthood functional limitations may be disrupted healthcare access. CLS involved youth often become disconnected from routine medical services and face gaps in health insurance coverage. This study examined whether CLS involvement before age 18 predicts functional limitations at age 29, and whether the observed relationship is totally or partially explained by reduced healthcare access during early adulthood.
2. Summary of Findings
The study revealed that different types of CLS involvement before age 18 affect functional limitations at age 29 through distinct pathways. Four key findings emerged:
First, youth arrested before age 18—even without incarceration—experienced higher rates of functional limitations at age 29 compared to those with no CLS contact (See Figure 1). This challenges assumptions that only incarceration produces lasting health harms, highlighting that arrest alone carries significant consequences.
Second, arrest and juvenile facility incarceration were associated with significantly reduced healthcare access during early adulthood (ages 18-28), including fewer years with health insurance, routine check-ups, and doctor visits when sick.
Third, reduced healthcare access served as a critical pathway linking arrest and juvenile incarceration to later functional limitations. For youth incarcerated in juvenile facilities, the relationship was entirely explained by diminished healthcare access. For arrested youth, healthcare access explained approximately 20-30% of the relationship.
Finally, youth incarcerated in adult facilities before age 18 showed a direct pathway to functional limitations not explained by healthcare access, suggesting that the experience itself—including exposure to violence, isolation, and developmentally inappropriate conditions—directly harms health in ways that persist into adulthood.
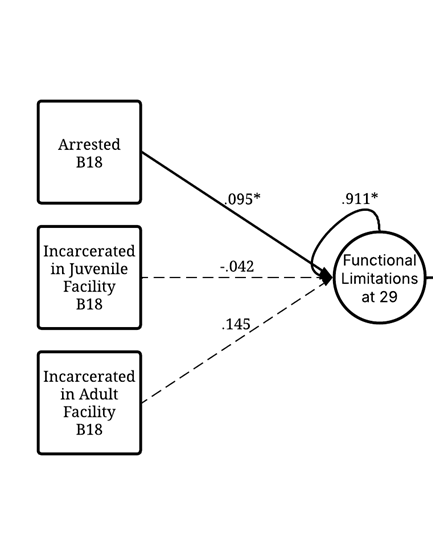
* p < .05 Notes: “B18” = Before 18
3. Implications
These findings, in conjunction with additional research, could help guide policies and practices for former CLS involved youth. The results suggest that even minimal CLS contact before 18 can set youth on a trajectory toward poorer health in adulthood, calling for policies to limit unnecessary CLS involvement and interventions that help CLS involved youth maintain a prosocial and healthy environment after involvement.
For policymakers, the findings support efforts to reduce unnecessary arrests and incarceration through diversion programs, restorative justice, and community-based alternatives. Given that arrest alone—regardless of subsequent incarceration—is associated with lasting health consequences, law enforcement and prosecutors should exercise restraint when deciding whether to arrest young people, particularly for non-violent offenses.
For healthcare systems, maintaining health insurance coverage and care continuity for system-involved youth is critical. The Consolidated Appropriations Act of 2023, which established new healthcare requirements for CLS-involved youth, represents a promising step. Healthcare coordinators who follow youth through system involvement and community reentry may be particularly valuable for ensuring care continuity.
For juvenile justice practitioners, these findings underscore treating health access as a core component of rehabilitation and reentry planning. Facilities should connect youth to health insurance before release and provide assistance navigating the healthcare system. The distinct pathways for different types of CLS involvement suggest interventions should be tailored: for arrested and juvenile-incarcerated youth, maintaining healthcare access is the top priority; for youth in adult facilities, additional trauma-informed interventions addressing unique harms may be necessary.
4. Data and Methods
This study analyzed data from the National Longitudinal Survey of Youth 1997 (NLSY97), a nationally representative study of 8,984 individuals born between 1980 and 1984 who were interviewed from 1997-2021. The analytical sample included 8,961 individuals who were under age 18 at baseline.
The primary outcome was functional limitations at age 29, measured through six questions about whether health problems limited physical activities, climbing stairs, work or daily activities, and social activities. Healthcare access was measured from ages 18-28 using years with health insurance, routine doctor check-ups, and doctor visits when sick.
CLS involvement was categorized into four groups: no contact, arrested only, arrested and incarcerated in a juvenile facility, and arrested and incarcerated in an adult facility before age 18. The analysis controlled for 28 confounding factors including demographics, parental characteristics, adverse childhood experiences, peer influences, school behaviors, and baseline health. Structural Equation Modeling was used to examine both direct effects of CLS involvement on functional limitations and indirect effects through healthcare access. Multiple sensitivity analyses supported the findings.
5. Conclusion
This study demonstrates that childhood involvement with the criminal legal system—including arrest alone—carries lasting consequences for functional limitations in early adulthood. The pathway from CLS involvement to functional limitations appears to operate through disrupted healthcare access, suggesting that maintaining care continuity for system-involved youth represents a concrete opportunity to mitigate long-term harms.
These findings call for coordinated action across pediatric healthcare, public health, and juvenile justice systems. By reducing unnecessary arrests and incarceration, maintaining health insurance coverage, and providing trauma-informed support, we can break the cycle linking childhood CLS involvement to adult functional limitations. Such efforts are essential for individual youth and for advancing health equity. Additional research is needed to test specific interventions, but the current evidence provides a strong foundation for future research on the health consequences of CLS involvement before 18 and policy action.
Disclosure: This research brief was prepared by Claud and reviewed/edited by Ian A. Silver.
